For many years doctors have told me that the best treatment for NAFLD/NASH (now referred to medically as MAFLD/MASH) was simply losing weight. That’s because we did not have any pharmaceutical treatments (until ezdiffra (resmetirom) from Madrigal in 2024), and until late stage fibrosis & cirrhosis develops, most liver disease is fully reversible.
On August 15, 2025, the FDA granted accelerated approval to Wegovy (semaglutide 2.4 mg) for treating adults with non-cirrhotic MASH and moderate to advanced liver fibrosis. This is an enormous milestone in the treatment of this disease. This makes Wegovy the first GLP‑1 receptor agonist to earn that distinction, and only the second overall drug to treat MASH.
GLP-1 drugs have obviously been all the rage for weight loss, and there has been some off-label use of them to treat liver disease like MASH, but in the Phase III ESSENCE trial, after 72 weeks, 63% of patients on Wegovy saw their steatohepatitis resolved without any worsening of fibrosis, compared to just 34% with placebo. And 37% saw an improvement in fibrosis with no worsening of inflammation, versus 22% in the placebo group. So it is not just helping patients lose weight but showing meaningful improvement for liver disease.
Dr. Martin Holst Lange, Novo Nordisk’s Chief Scientific Officer, put it bluntly: “Wegovy is now uniquely positioned as the first and only GLP‑1 treatment approved for MASH, complementing the already proven weight loss, cardiovascular benefits and extensive body of evidence linked to semaglutide”
Living with liver disease will still require lifestyle changes; these are foundational to the process. But now, there’s medicine that can resolve inflammation and heal fibrosis, beyond just nudging the scale downward. A tremendous step forward!
The energy in the room was electric. Packed to standing-room-only capacity, it held diverse representatives from nations as far afield as Qatar, Africa, and Brazil. These were not just academics or clinicians—they were heavy hitters in global health, some of whom had spent decades shaping the fight against diseases like HIV, malaria, and obesity. And yet, amidst this impressive gathering, a dark truth emerged: our healthcare system is failing millions of people with fatty liver diseases, including Non-Alcoholic Fatty Liver Disease (NAFLD) and its more severe form, Non-Alcoholic Steatohepatitis (NASH).
Dr. Christoph Benn, an influential early leader of the world-renowned Global Fund, did not mince words. During the discussion, he bluntly stated that until invited to this event, he’d never heard of NAFLD or NASH—not by these names, nor by their newer terminology, MASLD and MASH. His message was painfully clear: if a disease impacts an estimated 100 million Americans and remains largely invisible on the global stage, then the system designed to promote awareness and action has failed. What’s more, the 2024 Lancet publication on global health—an agenda-setting document for the next decade that for the first time is making a major shift from infectious diseases to non-communicable diseases (NCDs) —makes no mention of liver disease at all. Zero.
Let that sink in. Our healthcare policymakers are flying blind on an epidemic of massive proportions.
“100 million Americans are impacted by NAFLD, yet it remains invisible on the global stage.”
It was late September 2024, and for the first time in history there was a United Nations General Assembly (UNGA) sidelines event focused on liver disease, specifically MAFLD/MASH. UNGA Week is an important series of side events that include panel discussions, focus groups, and gatherings of global leaders and experts, often taking place in parallel to the formal UNGA sessions and are organized by UN member states, UN agencies, non-governmental organizations (NGOs), and private sector groups. These UNGA sidelines are key opportunities for advocacy, coalition-building, and policy discussions on pressing global issues like health, climate change, education, and sustainable development.
I have attended many NASH-related conferences and panel discussions in the years since I started NASHAWARE and began working with ALF, but they were also from a US-centric standpoint, and so the global viewpoints that were expressed during this amazing UNGA session hosted by The Economist Impact were refreshing and invigorating. The real eye-opener for me was how far we really have to go to make an impact in global health policy. You may have thought that with NASH drugs being a hot multi-billion dollar industry that there would be at least some action on the policy front, but other than ALF’s recent success in helping secure funding for the first US government-funded NAFLD study there really hasn’t been anything of note, and as the participants pointed out, plenty of missed opportunities.
The stakes have ever been higher or more clear, as illustrated by a sobering statistic from Dr. Arun Sanyal. “When a person shows up a emergency room for the first time with a complication of cirrhosis, two out of three individuals, it is the first day their liver disease has been diagnosed.” This is not just an oversight; it’s a systemic failure—a glaring indictment of our approach to prevention, early detection, and education. As Dr. Jeffrey Lazarus put it: “For everyone working in public health, global health, even health economics…it’s not that we’re not on their agenda. Some of them don’t even know this disease exists.”
For 20 or more years, the entire healthcare system has failed that patient.” – Dr. Arun Sanyal
Globally, countries like Qatar offer a blueprint for action. Their Minister of Health, Her Excellency Al Kuwari, spoke about how liver testing has been integrated into national health screenings. By embedding obesity and diabetes monitoring into the fight against liver disease, Qatar has not only halted the growth of obesity but also set a bold target to reduce it by 8% by 2030. “Yes we need to continue to study this, but we have enough data to take action” she declared. While they have the benefit of a small and affluent population, they can still inspire other nations through action.
Johanna Ralston, CEO of the World Obesity Foundation, made the observation that NAFLD is both “everywhere and nowhere.” Her point was clear: the disease is ubiquitous, affecting millions, yet remains absent from critical discussions on high-priority non-communicable diseases by organizations like the WHO. “It’s an exciting time for all of us working in this metabolic health space,” she mentioned, highlighting the ways that all of the various disease communities are coming together. “The timing is now,” Dr Sanyal added, echoing the call for action and collaboration to combat this invisible epidemic.
Contrast this with the fragmented and often lethargic approach in the U.S., where red tape, special interests, and stigma hinder progress. For instance, stigma around liver diseases being linked to alcohol persists, leading to misconceptions even within families. This stigma discourages both patients and policymakers from engaging in meaningful discussions, let alone action. We are also facing an uphill battle on messaging, which is hindered by a lack of clear and concise messages, even around the basic facts like what to call it (several panelists misstated the new terminology). Advocacy groups like the American Liver Foundation are pushing against this tide but are hindered by limited budgets and an uphill battle for donor dollars.
So, what’s the solution? The answer lies in disruptive advocacy—moving beyond just raising awareness to shaking the very foundations of our healthcare and political systems. As a former UK NHS legal counsel argued at the event, awareness campaigns often fall victim to shifting political winds. Instead, we must demand accountability by presenting stark, undeniable truths: “The healthcare system is failing millions of Americans. Here are the X lives lost and Y economic costs of inaction. Here’s what we need to fix it, and here’s how politicians can be remembered for saving lives, not abandoning them.”
It’s also about partnership and focus. We need to stop seeing liver disease in isolation and address the elephant in the room: metabolic dysfunction. NAFLD and NASH are intrinsically tied to obesity, diabetes, and poor nutrition. Advocacy must break through silos and unite stakeholders across fields—from obesity-focused NGOs to diabetes organizations—to tackle the root causes. As one speaker put it, we need to see “the elephant in the room, not the individual trunk or legs.”
The medical community must also adapt its approach to address the growing burden of NAFLD and NASH. Overspecialization within healthcare often creates silos that hinder a comprehensive approach to these diseases. Specialists in hepatology, gastroenterology, endocrinology, and cardiology need to collaborate more effectively, sharing knowledge and resources to tackle the interconnected nature of metabolic dysfunction. Medical training and research funding must emphasize cross-disciplinary education and solutions, ensuring that future healthcare providers are equipped to address these complex, multifaceted conditions.
Yet even the most compelling arguments won’t resonate without clarity of messaging. Attendees mentioned using visuals that elicit emotional responses; imagine a basketball court: ten kids playing a game. Now imagine telling those watching that one of these kids will develop MASLD or MASH before adulthood. One in ten. That’s the kind of visceral imagery we need to cut through the noise and make statistics real.
And then there’s the power of technology. A young doctor from Africa highlighted how AI tools could amplify these efforts, from translating advocacy materials into multiple languages to identifying high-risk individuals. These tools are there; we just need the vision and will to use them.
The harsh reality is that the healthcare system—both in the U.S. and globally—has left millions to fall through the cracks. But we can change this narrative. By simplifying our message, demanding specific actions, and rallying patients, advocates, and healthcare professionals to disrupt the status quo, we can force the system to do better.
Because the stakes are too high, and the cost of inaction is measured in lives lost—a price we cannot afford to keep paying.
(The entire very informative event can be viewed here.)
Last night French biotech company Genfit released the results of their widely anticipated Phase III study on Elafibranor, a NASH therapeutic that had shown tremendous promise in earlier trials.
Unfortunately, the trial failed to meet both the primary and secondary endpoints. The treated patients response wasn’t statistically meaningful versus the placebo control group. Genfit’s CEO Pascal Prigent said “These results are highly disappointing.” The stock is down by over 65% today.
This setback leaves us with just Abbvie’s cenicriviroc study to look forward to this year, due in late 2020 if there are no delays due to the Covid crisis. Intercept’s Ocaliva is due for FDA approval soon, but seems to have limited effectiveness in specific NASH cases.
The best treatment for NASH and NAFLD remains a healthy diet and lifetsytle changes for the foreseeable future.
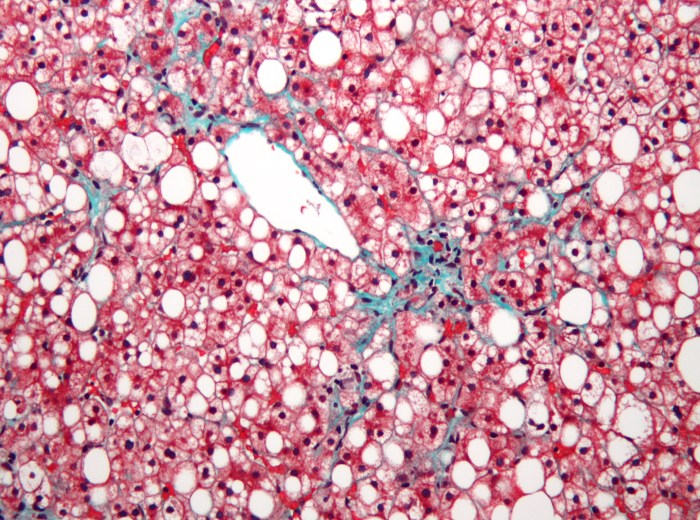
One of the questions I see asked all of the time is what kind of testing is the best to determine if someone has NASH. I’ve written about the challenge of diagnosis before, but there are a lot of scared individuals out there trying to get answers from their under-educated primary case physicians, and everyone wants to skip the preliminary steps and go straight to a definitive diagnosis. If only it were that easy!
For the 2nd International NASH Day yesterday I took part in a webinar along with Dr. Tuan Pham of the University of Utah. Dr. Pham gave a great overview of the latest in the NASH space and I shared the story of my mom to provide an advocate perspective.
For #NASHDAY I’m asking everyone I know to “Give It Up” for NASH Awareness. It could be sugar, coffee, alcohol, TV, politics…literally anything! Write about what you are giving up on the sign attached and share it all over social media next Wednesday June 12th to help spread the word.
And if you can take the $5 that would have gotten you a cup of coffee and instead donate it to the American Liver Foundation’s NASH Day page, you can help raise awareness, provide education and support, and help fund treatments for NASH patients in the future.
A few months ago I was honored to take part in an American Liver Foundation effort to educate and raise awareness for NASH. I travelled to University of San Diego’s Altman Clincial and Translational Research Institute where I recorded a video telling my mom’s story so that others could learn and benefit from our loss. I was joined by a panel of individuals currently living with various stages of NASH and a few distinquished medical experts in the field.
The videos are finally being released as part of our leadup to the 2nd International NASH Day on June 12th. You can watch the entire video below.
For #NASHDAY I’m asking everyone I know to “Give It Up” for NASH Awareness. It could be sugar, coffee, alcohol, TV…literally anything. Post about what you are giving up on social media to help spread the word. And if you can take the $5 that would have gotten you a cup of coffee and instead donate it to the American Liver Foundation’s NASH Day page, you can help raise awareness, provide education and support, and help fund treatments for NASH patients in the future.
Will move for approval in US and Europe later this year
Eagerly awaited Phase 3 trial results were released early Tuesday morning from Intercept Pharmaceuticals, showing positive results for the study’s primary goal of showing a statistically significant reduction in liver fibrosis compared to placebo. As a result, Intercept will seek approval in the US and Europe to permit the drug, known as Ocaliva, to be used as the first ever treatment for NASH-related fibrosis. The stock price rose as high as 23% on the news.
I have a friend who once lost a whole bunch of weight by removing two simple things from his diet. Cheese and soda. This was well before the current Paleo diet craze, when sugary drink taxes weren’t even whispered in the most progressive of city councils. It was also well before I knew anything about the liver or the difference between sucrose and fructose in the sugar I consumed. His story always stuck with me, though I never realized why it had worked.
Ever since the untimely death of my mother from NASH, I have spent a lot of time learning about the underlying causes that likely led to her liver failure. Along the way, I had to reexamine a number of misconceptions and prejudicies I’ve had about health and eating. Whether from genetics or pure luck, I’ve been blessed all my life with never having to worry about weight or what I eat. I never put a lot of thought about what I was putting inside my body until i started to read research about how obesity and metabolic syndrome developed, and why we were suddenly facing a worsening crisis over the last 50 years.
What I’ve found has changed my entire view on food & health.